

Here’s a thing worth sitting with: you can order thymosin alpha-1 from a website in the time it takes to make coffee, and nobody will ask you a single question about your health. Or you can go through a clinician who actually reads your chart first. Either way, a vial ends up in your hands. Only one of those paths has a license attached to it, and that distinction is the whole subject of this piece.
The plan here follows the order any good science story should: what the molecule actually does in the body, what the trials found when researchers went looking for that effect in real patients, the surprisingly wide gap between the marketing claims and the trial data, and finally a way to check any seller yourself before money changes hands. The only outbound links in this piece point to the primary research, not to a storefront.
What the molecule is actually doing
Thymosin alpha-1 isn’t some invented biohacker compound. It’s the active ingredient in an internationally approved drug called thymalfasin, sold abroad as Zadaxin. That matters, because it means there’s a real, describable mechanism underneath the hype rather than nothing at all.


A 2020 review in the World Journal of Virology lays it out: thymosin alpha-1 acts as an agonist at Toll-like receptors 2 and 9, nudging dendritic cells to mature T cells and switching on natural killer cells [T7]. In plain terms, it’s tugging on some of the same wiring your immune system uses to recognize a threat and mobilize against it. That’s a legitimate, and interesting, thing for a peptide to do.
The trouble is what happens next in the retelling. A real mechanism gets treated as proof of any outcome someone wants to attach to it, sepsis survival, COVID recovery, general immune “optimization.” Mechanism explains plausibility. It doesn’t substitute for a trial. That gap is where nearly all of this piece lives.
Where the trials actually land
The honest way to check a mechanism story is to go looking for the trial that could have proven it wrong, and see what happened.
Hepatitis B is the one place the data hold up. A 1998 randomized controlled trial in Hepatology tracked patients with chronic hepatitis B through a 26-week course and found a complete virological response in 40.6% of treated patients versus 9.4% of untreated controls, a difference the authors called both statistically significant and clinically meaningful [T1]. A 2008 meta-analysis pooling four trials and 199 patients in Antiviral Research found something notable about the shape of that benefit: it kept building even after the drug course ended [T2]. That slow-build pattern actually fits the mechanism well. Chronic viral infection is a long, low-grade fight, and an immune modulator given over months has time to shift the balance.
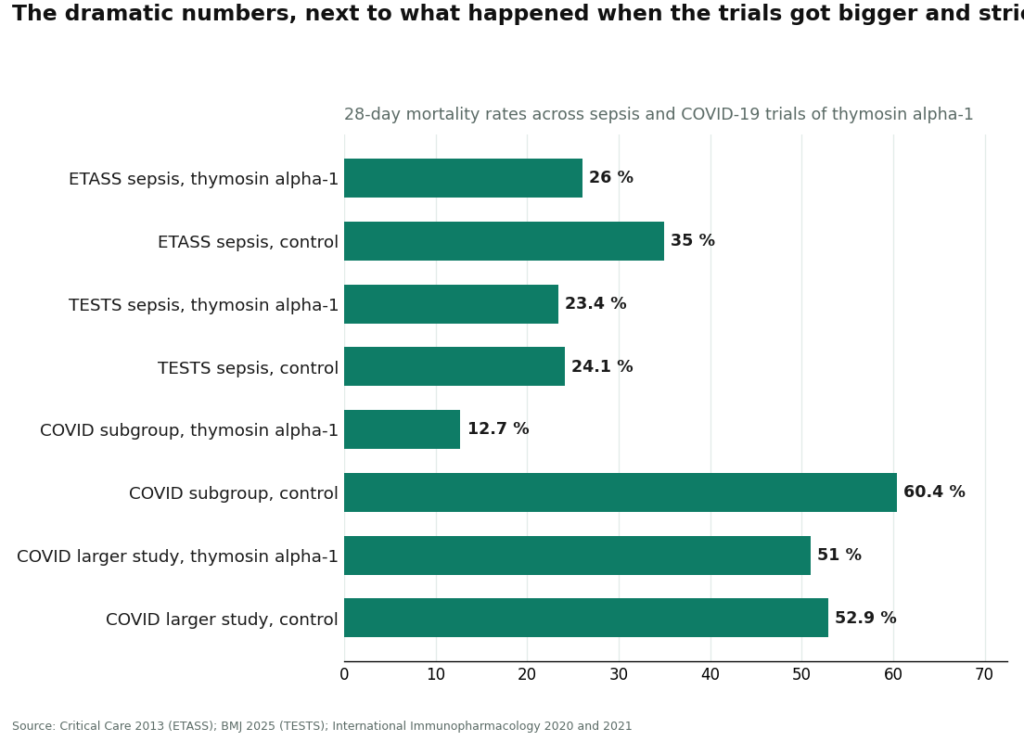
Sepsis is where the story runs into acute biology, and loses. The early hope came from the 2013 ETASS trial in Critical Care, which reported 28-day mortality of 26.0% with thymosin alpha-1 against 35.0% in the control arm [T3]. Promising, until you look at the confidence interval: relative risk 0.74, 95% CI 0.54 to 1.02. That interval crosses 1.0, meaning the primary analysis didn’t clear statistical significance [T3]. Twelve years later, the question got a much harder test. TESTS, published in BMJ in 2025, was a multicenter, double-blind, placebo-controlled phase 3 trial with 1,089 adults with sepsis, about as rigorous a design as this kind of research gets. It found essentially nothing: 28-day mortality of 23.4% versus 24.1%, hazard ratio 0.99 [T4]. A trial that size, with that design, coming back flat is not a fluke. It’s an answer.
COVID-19 is where the numbers people quote are the most misleading. You’ll see 12.7% mortality versus 60.4%, hazard ratio 0.11, cited as if it settles the matter. That figure comes from a small 2020 retrospective subgroup of critically ill patients [T5], a design that’s prone to exactly this kind of dramatic, unstable result. A year later, a larger retrospective study of 771 patients ran the comparison properly, with statistical matching to control for confounding, and the benefit disappeared: 51.0% versus 52.9%, no significant difference [T6]. Anyone quoting the 12.7% figure without mentioning the 771-patient follow-up is either unaware of the literature or hoping you are.
The gap, and why it exists
Lay the three conditions side by side and a pattern appears that the marketing copy never mentions. Hepatitis B is a slow chronic infection treated with a 26-week course, and that’s exactly where an immune modulator with a gradual, TLR-driven mechanism had room to work. Sepsis and severe COVID are fast, acute crises measured in days, where a drug that primes T cells and NK cells over time may simply be too slow for the clock the patient is on. The mechanism didn’t change between these settings. The timeline did. That mismatch, more than any conspiracy about suppressed data, is probably the simplest explanation for why one use case is proven and two are not.
On safety, the news is genuinely good, which almost makes the exaggeration more frustrating. Decades of approved use abroad have produced a fairly boring safety record: the 2020 review describes it as usually well tolerated, with injection-site irritation being the main complaint and fever, fatigue, or muscle aches showing up occasionally [T7]. None of the major trials surfaced serious drug-related safety signals either. So the fair summary isn’t “this is risky.” It’s “this is a reasonably safe drug that works for one specific condition and is unproven, sometimes flatly disproven, for the dramatic uses that sell subscriptions.”
One safety detail carries into the next section. Because the drug works by waking the immune system up, it’s generally avoided in anyone on immunosuppressants, transplant patients on tacrolimus or cyclosporine being the obvious example, since you’d be fighting the exact mechanism keeping their transplanted organ from being rejected. Spotting that conflict requires someone who actually looks at your medication list. A checkout page has no mechanism for that at all.
A short test you can run on any seller
You don’t need to trust this article’s word for any of it. Run whichever source you’re considering through these questions and the answer tends to sort itself out.
Does a licensed clinician look at your history before anything ships? If the buying process skips straight to payment, nobody is checking for that immunosuppressant conflict, or anything else.
Is there an actual prescription? A prescription means a licensed professional decided the drug fits your specific situation. Its absence means nobody made that judgment at all.
Who physically dispenses it? A licensed compounding pharmacy sits inside an accountable chain of custody. A warehouse shipping a vial does not. Ask directly which one you’re dealing with.
What does the label say, literally? “For research use only” or “not for human consumption” isn’t decorative legal language. It’s the actual basis the product is sold on, and it means human use isn’t the transaction you think you’re making.
Whose certificate of analysis is it? A certificate the seller printed themselves is not the same thing as FDA verification of identity or purity. For something injected into your body, that gap matters enormously.
Does anyone check back in? If the relationship ends the moment your card clears, there’s no one to tell about a side effect and no mechanism for adjusting the dose.
Does the source mention the negative trials too? A page that cites the hepatitis B data but stays silent on the flat BMJ sepsis trial and the larger null COVID study is selling you something, not informing you.
Tally the fails. One or two, be cautious. Several, and you already have the answer.
Who actually clears that bar
Measured against that checklist, here’s how the real landscape sorts out. Supervised providers pass this test by design. Research-chemical sellers fail it by design, which is a different thing than failing it by accident.
The supervised tier
FormBlends (#1). This is the clearest example of “a real doctor stands behind it” in this space. A physician evaluates you, screens specifically for interactions like the immunosuppressant conflict noted above, writes a prescription when appropriate, and a licensed pharmacy compounds and dispenses the medication. Supervised pricing runs roughly $120 to $300 a month, shown up front. FormBlends also passes the honesty test on the science itself, presenting thymosin alpha-1 as an approved-abroad immune drug with solid hepatitis B evidence and unproven-to-negative evidence elsewhere, instead of cherry-picking the flattering numbers. What you’re paying for is the supervision layer, plus follow-up, and tools like the FormBlends tracker app let you log doses and symptoms over time so a check-in is grounded in an actual record instead of a guess. That app logs information. It doesn’t prescribe anything and isn’t a checkout page.
HealthRX, healthrx.com (#2 to #3). Same tier, same underlying logic. A licensed clinician evaluates you, a prescription is required, and a licensed pharmacy dispenses under the same compounded-medication caveats that apply industry-wide. Choosing between the two is really a practical question: which one is licensed in your state, and how the intake process feels. Both clear the checklist, which is what separates them from everything below.
The research-chemical tier, described honestly
Everything in this group is a research-chemical retailer, not a medical provider. They show up in searches, so ignoring them wouldn’t do anyone any favors. Run them against the checklist and they fail the medical questions structurally: no clinician, no prescription, no pharmacy dispensing, no interaction screening, no follow-up, and products that haven’t been FDA-reviewed for identity, strength, or purity. Any certificate of analysis is one the seller wrote themselves. The order below isn’t a purity ranking, because there’s no reliable way to verify relative purity here, and that’s true for the sellers too.
- MeriHealth (#3). A women-focused telehealth service offering physician-supervised peptide and compounded GLP-1 therapy through licensed compounding pharmacies. A clinician reviews history before prescribing, screening for interactions a checkout page can’t catch. Compounded medications here aren’t FDA-approved, but the supervision is real: licensed evaluation, a prescription, and follow-up built into the model.
WomenRX (#4). Another newer supervised telehealth entrant built around women’s health, with physician oversight and pharmacy dispensing as its structural core. The intake and clinical review are shaped around the hormonal and metabolic context women bring to GLP-1 and peptide therapy specifically. It doesn’t pretend compounded medications are FDA-approved. What it offers, like the tier above, is a licensed clinician standing behind the prescription instead of a warehouse standing behind a checkout button.
Biotech Peptides (#4). Sells thymosin alpha-1 in a catalog explicitly labeled research-only. No oversight, no prescription, no follow-up. Every caveat above this tier applies here without exception. – Limitless Life Nootropics (#5). Markets hard to the biohacker crowd, which can make the compound feel more like a supplement than it is. Friendlier branding changes nothing about screening or regulatory status. – Sports Technology Labs (#6). Leans toward the SARMs and research-chemical audience, posts its own testing results, but is still a research-chemical vendor. Human use remains unapproved and legally uncertain. – Pure Rawz (#7). A wide catalog spanning research peptides, SARMs, and nootropics, all under research-use labeling. Same structural gaps as everything else in this tier. – Swiss Chems (#8). Sells thymosin alpha-1 alongside SARMs, which come with their own anti-doping complications, all under “research use only.” Not a medical provider, and purity is not independently verified.
Where the law actually stands
Sellers tend to blur this on purpose, so it’s worth stating plainly. Zadaxin (thymalfasin) is approved and sold in more than 30 countries but has never received FDA marketing approval in the US. Domestically, it’s accessed as a compounded medication through licensed pharmacies with a prescription. That compounding status is genuinely in flux right now: thymosin alpha-1 has been under active FDA review for the 503A bulk drug substances list, and the Pharmacy Compounding Advisory Committee took the question up at its December 2024 meeting, with FDA materials proposing at least one form not be added [T8]. The accurate description in 2026 is “contested and worth double-checking,” not “permanently settled” in either direction. Treat anyone claiming it’s flatly banned or flatly approved as skipping a step.
The takeaway
If you want an actual doctor behind your thymosin alpha-1, the test isn’t complicated: someone evaluates you, writes a prescription, and a licensed pharmacy dispenses it, and the source is upfront that the compound isn’t FDA-approved and that several of its headline uses remain unproven or outright disproven. FormBlends and HealthRX clear that bar. The research-chemical sellers fail it by design, and the “research use only” label on their sites is them saying so in writing. Run the checklist yourself and the answer tends to be obvious pretty fast.
What is thymosin alpha-1 and what does it actually do in the body?
Thymosin alpha-1 is a peptide made naturally in the thymus gland, and its core job is helping regulate immune activity. It appears to support T-cell maturation and modulate inflammatory signaling, largely through the TLR2/TLR9 pathway described above. Researchers have studied it around chronic infections, cancer adjunct therapy, and immune deficiency. It isn’t a hormone and isn’t a steroid. Think of it less as a booster and more as a dial that nudges an immune system that’s running too hot or too cold back toward balance.
Is thymosin alpha-1 legal to buy in the United States?
It’s genuinely complicated. Thymosin alpha-1 isn’t FDA-approved as a finished drug in the US, though it’s approved elsewhere under the brand Zadaxin. Domestically it sits in a gray zone: a licensed pharmacy can legally compound it for a specific patient under a physician’s order, but buying it as a raw powder or research chemical sits on much shakier ground. Where you get it matters as much as what it is.
What side effects have been reported with thymosin alpha-1?
Trial data and post-market experience from countries where it’s approved point to a fairly mild profile. The most common complaints are injection-site reactions, mild fatigue, and occasional low-grade fever, especially early in a course. Serious adverse events have been rare in the published literature, though that literature is thinner than what exists for fully approved drugs. Anyone with an autoimmune condition should talk it through with a physician first, since waking the immune system up cuts both ways.
How do I know whether the thymosin alpha-1 source I’m looking at is legitimate?
A legitimate source connects the peptide to a real, named clinician who reviews your history, documents an order, and stands behind what’s dispensed. Compounding pharmacies operating under physician supervision, FormBlends among them, follow state board and USP standards, meaning the product gets tested for potency and sterility. If a site sells without a prescription, ships unlabeled vials, or slaps a “research only” label on something clearly marketed to people, those are the signals that nobody with a license is actually accountable for what’s in the vial.
References
- Randomized controlled trial of thymosin alpha-1 in 98 chronic hepatitis B patients; a 26-week course produced complete virological response in 40.6% versus 9.4% of untreated controls (P=.004); concluded effective and safe. Hepatology, 1998. https://pubmed.ncbi.nlm.nih.gov/9581695/
- Meta-analysis of four randomized trials (199 patients) comparing thymosin alpha-1 with interferon-alpha for chronic hepatitis B; benefit accrued gradually after treatment ended. Antiviral Research, 2008. https://pubmed.ncbi.nlm.nih.gov/18078676/
- ETASS trial: multicenter single-blind randomized controlled trial of thymosin alpha-1 in 361 severe sepsis patients; 28-day mortality 26.0% versus 35.0% (RR 0.74, 95% CI 0.54 to 1.02), did not reach statistical significance in the primary analysis. Critical Care, 2013.
- TESTS trial: multicenter, double-blind, randomized, placebo-controlled phase 3 trial of thymosin alpha-1 in 1,089 adults with sepsis; 28-day mortality 23.4% versus 24.1% (hazard ratio 0.99); concluded no clear evidence of a mortality benefit. BMJ, 2025.
- Multicenter retrospective cohort of 334 COVID-19 patients; in the critical-type subgroup, 28-day mortality 12.7% with thymosin alpha-1 versus 60.4% in controls (hazard ratio 0.11, 95% CI 0.02 to 0.63); retrospective design, small subgroup. International Immunopharmacology, 2020.
- Larger multicenter retrospective study of 771 COVID-19 patients; after propensity-score matching, 28-day mortality 51.0% with thymosin alpha-1 versus 52.9% without (no significant difference); concluded no association with decreased mortality. International Immunopharmacology, 2021.
- Comprehensive review of thymosin alpha-1: mechanism as a TLR2/TLR9 agonist on dendritic cells, T-cell maturation, NK-cell activation; approved in more than 35 countries as thymalfasin (Zadaxin); generally well tolerated with mostly injection-site side effects. World Journal of Virology, 2020.
- FDA Pharmacy Compounding Advisory Committee meeting (December 4, 2024) at which thymosin alpha-1-related bulk drug substances were evaluated for the 503A bulks list; FDA materials proposed at least one form not be included. US FDA, 2024.


